

Parathyroid Surgery
What are the parathyroid glands?
Parathyroid glands are small but essential glands located in your neck that play a crucial role in regulating and controlling calcium levels within your body. In a healthy individual, there are typically four parathyroid glands situated in close proximity to your thyroid gland. Generally, there are two glands on each side of your neck, located just behind it. These glands are relatively small, measuring normally about 5-7 millimeters in size and weighing approximately 30-60 milligrams. They have a distinctive yellow-tan appearance that can be recognized during medical evaluations. These vital glands manage calcium levels in your body through the production of two important hormones: Parathyroid Hormone (PTH), which functions to increase calcium levels, and Calcitonin, which works to reduce calcium levels in the bloodstream.

What is hyperparathyroidism (HPT)?
Hyperparathyroidism is a medical condition that occurs when one or more of the parathyroid glands become overactive, leading to the excessive production of Parathyroid Hormone (PTH). This overproduction of PTH results in an elevation of calcium levels in the blood, which can lead to a variety of side effects and complications. Some of these potential side effects include osteoporosis, which weakens bones, kidney stones that can cause significant discomfort, constipation, and increased thirst, all of which can negatively impact a person's overall health and quality of life.
What are the types of hyperparathyroidism (HPT).
There are three types of hyperparathyroidism, each with different causes and treatments:
Primary Hyperparathyroidism (pHPT)
Secondary Hyperparathyroidism (sHPT)
Tertiary Hyperparathyroidism (tHPT)
Primary Hyperparathyroidism (pHPT)
This is the most common type, usually caused by one gland becoming overactive. A tumor called an adenoma (benign) forms in this gland, leading to too much parathyroid hormone (PTH) being made. The extra hormone signals the body to raise calcium levels. Even with high calcium, the gland doesn't react to normal controls and keeps producing PTH, which raises calcium even more, causing various health issues.
The cause of pHPT is due to:
Single adenoma – 85%
Hyperplasia (enlargement) – 10%.
Multiple adenoma – 5%.
Cancer <1%.
Secondary Hyperparathyroidism (sHPT)
Secondary hyperparathyroidism happens in patients with kidney disease who lose a lot of calcium through urine. To cope with this loss, the parathyroid glands grow larger. All glands are affected in this condition. Doctors treating kidney disease try to manage the calcium loss with medication, but there is a limit to how much the gland enlargement can be controlled. Eventually, about 5% of cases need surgery. The surgery involves removing all parathyroid glands and re-implanting half of one into the muscles of the neck or the arm.
Tertiary Hyperparthyroidism (tHPT)
Tertiary hyperparathyroidism occurs when parathyroid glands become overactive due to long-term stimulation from chronic kidney disease or vitamin D deficiency. In response to low calcium or high phosphate levels, these glands secrete excess parathyroid hormone (PTH), causing elevated blood calcium levels and symptoms like weakness, fatigue, kidney stones, and bone pain. Unlike primary or secondary hyperparathyroidism, it often requires surgery to remove the overactive glands, particularly in severe cases. Effective diagnosis and treatment are crucial for management.
What problems can high calcium cause?
Calcium levels are typically tightly controlled. Hyperparathyroidism raises calcium levels, which can cause various symptoms. Many individuals may not be aware of their high calcium. However, increased PTH and calcium can lead to symptoms that affect multiple body systems.
Serious issues from high calcium that may require surgery include:
Kidney stones
Osteoporosis
Irregular heartbeats from very high calcium
High PTH and calcium can also caused various other issues, including:
Fatigue, memory loss and irritability.
Excessive thirst.
Constipation and abdominal pains.
Excessive urination.
Do I have Parathyroid Cancer?
The simple answer is almost certainly NOT. Parathyroid cancer is extremely rare. In fact, less than 1% of all cases of hyperparathyroidism can be attributed to the presence of a cancerous growth. Rather, most instances of primary hyperparathyroidism arise from a specific type of tumor known as an adenoma. An adenoma is classified as a benign tumor, meaning it does not possess the ability to invade surrounding tissues or spread throughout the body, which distinguishes it from malignant tumors, the type associated with dangerous cancers. Often, an adenoma can lead to significant enlargement of the gland itself, growing to a size that is two to ten times larger than what is considered normal. The primary issues that arise from this condition stem from the excessive secretion of parathyroid hormone (PTH), which results in elevated levels of calcium in the bloodstream, ultimately leading to various health complications.
How is Hyperparathyroidism diagnosed?
Several tests are typically required if primary hyperparathyroidism is being considered as a possible diagnosis. In most patients, the diagnosis is often suspected due to the presence of elevated calcium and parathyroid hormone (PTH) levels, which may be found accidentally during an investigation for other unrelated medical reasons. The necessary investigations can be systematically broken up into two key components, allowing for a more organized approach to diagnosis and treatment.
Tests to confirm the diagnosis (Biochemistry)
Calcium level.
PTH level.
Vitamin D level – a low vitamin D can elevate your PTH level.
Urine Test - 24-hour collection of urine to check calcium levels which should be high.
Parathyroid Venous Sampling
Tests to locate the abnormal gland
Neck Ultrasound
Sestamibi scan.
4DCT - Neck/parathyroids
Neck Ultrasound
A parathyroid ultrasound is a non-invasive imaging technique for evaluating the parathyroid glands, which regulate calcium levels. It uses high-frequency sound waves to create detailed images that help identify abnormalities like enlargement or tumors, aiding in diagnosing conditions such as primary hyperparathyroidism and assessing surgical needs. The quick, painless procedure involves no radiation, making it safe for patients, and provides real-time images to guide treatment plans.

Sestamibi Scan
A sestambi is a specialized parathyroid scan in which you will be receiving a very small amount of a radioactive labelled injection. This radioactive material is designed to be absorbed by the abnormal parathyroid gland, allowing it to be clearly visualized on the scan. As a result, this imaging technique will confirm whether the enlarged gland observed on ultrasound is, in fact, overactive.

4D CT Parathyroids
4D CT parathyroid imaging is an advanced technique that precisely locates and assesses parathyroid glands. The "4D" element adds time as a dimension, enabling dynamic imaging of blood flow and gland function. This method effectively identifies parathyroid adenomas and hyperplasia linked to hyperparathyroidism. By offering detailed anatomical and functional insights, 4D CT aids surgeons in planning interventions, enhancing surgical outcomes, and reducing complications. It is essential for the preoperative assessment of suspected parathyroid disorders.
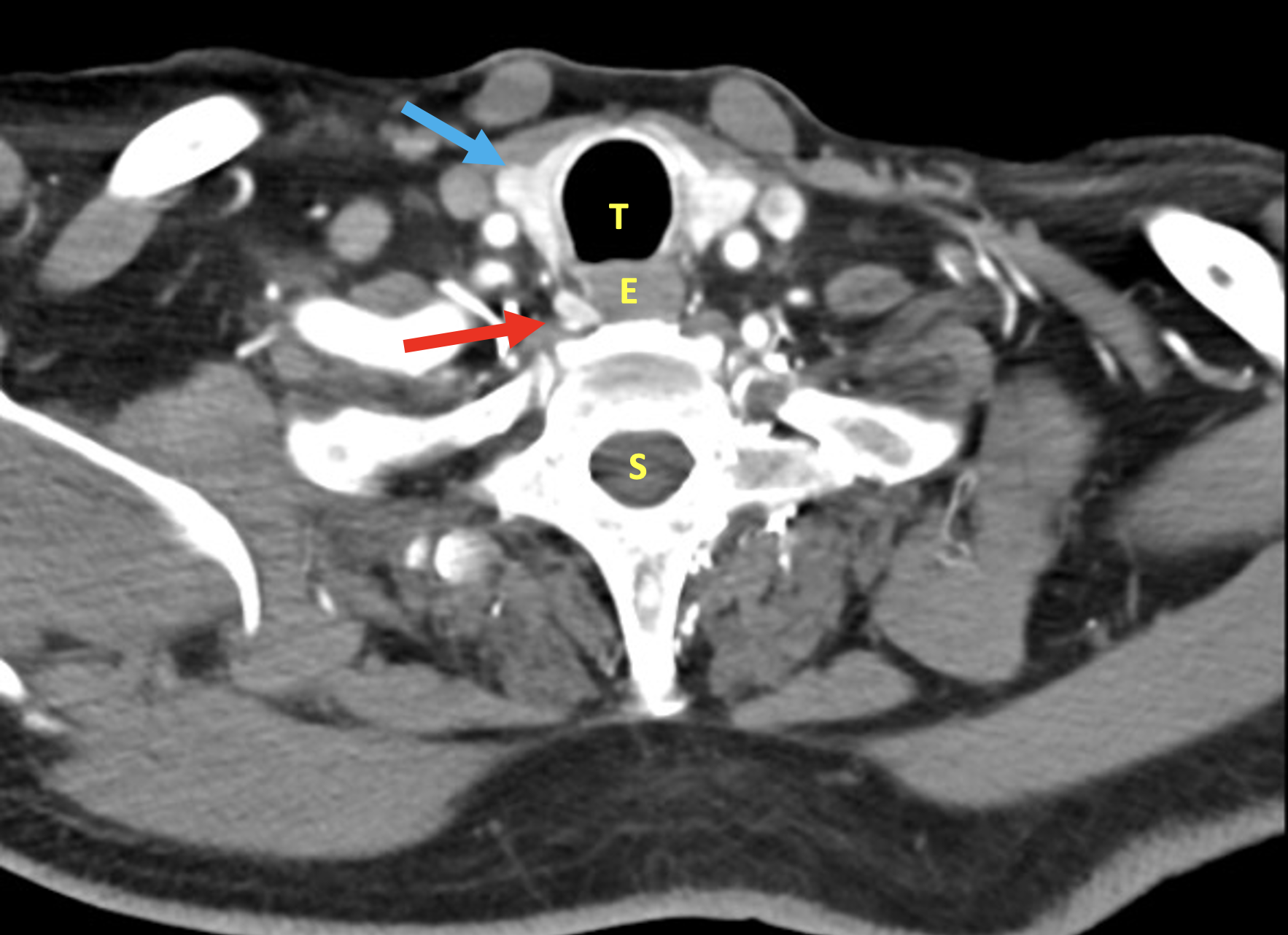
4DCT - Red arrow shows abnormal parathyroid gland. Blue arrow shows thyroid gland
T= Trachea, E=Oesophagus, S=Spine
What is a parathyroidectomy procedure?
A parathyroidectomy is the procedure to remove an abnormal parathyroid gland. There are two main types of parathyroid surgery:
Minimally Invasive Parathyroidectomy (MIPS)
Bilateral neck Exploration (BNE)
Minimally Invasive Parathyroidectomy (MIPS)
This procedure removes an enlarged overactive parathyroid gland through a small incision (less than 2 cm). It's suitable for about 85% of patients. The benefits include a small cut that heals well for a better appearance and minimal disruption to the neck tissue, promoting quicker recovery and less internal scarring. A focused Minimal Invasive Parathyroid Surgery (MIPS) is done when the abnormal gland's exact location is known before surgery. This method uses a small incision and creates a direct tunnel to the gland. Although technically challenging, it has become the standard approach for removing identifiable parathyroid glands.
Bilateral Neck Exploration (BNE)
If the abnormal gland cannot be successfully located during pre-surgery scans, it will then be necessary for both sides of the neck to be thoroughly examined during the surgical procedure. It is often essential to locate all four parathyroid glands to effectively identify which gland is abnormal. This important surgical procedure is referred to as Bilateral Neck Exploration (BNE). A BNE typically involves a surgical incision measuring 3-5 cm, along with more extensive surgical techniques, which can lead to additional scarring and some increased discomfort following the operation. Ultimately, both Minimally Invasive Parathyroid Surgery (MIPS) and Bilateral Neck Exploration (BNE) have similar recovery times and associated risks for patients.
What is involved in a parathyroidectomy operation?
A parathyroidectomy can be done using a minimally invasive method (MIPS) or a bilateral neck exploration (BNE). You will need general anesthesia and will stay overnight in the hospital. The surgery usually lasts between 30 minutes and 2 hours, depending on how difficult it is to find the abnormal gland.
When you arrive, you will meet the anesthetist, and a drip will be placed in your hand to put you to sleep. Both methods involve a small cut in your neck to access the abnormal gland. Once found, the gland will be removed and checked by a pathologist while you are asleep, which is called a Frozen Section.
After surgery, your wound will be closed with dissolving stitches and covered with a plastic strip. For detailed post-operative care, refer to the Post-operative advice section. You can eat and drink as you like once back in your ward, but you may have a sore throat that can be treated with simple pain relief medication. A blood test the next morning will confirm the success of the surgery.
When is a Minimally Invasive Parathyroidectomy (MIPS) performed?
Not everyone can have a parathyroidectomy through a small (<2cm) incision. In 85% of cases, the abnormal gland can be identified using pre-operative images. However, if the gland's location is unclear, a larger incision is needed to examine both sides of the neck. In these instances, all four parathyroid glands must be located to find the abnormal one, requiring a more extensive procedure, known as Bilateral Neck Exploration (BNE), making MIPS unsuitable. Dr. Green will advise you before your surgery on whether MIPS is an option or if a full neck exploration is necessary.
When will I know the operation has been successful?
After your operation, Dr. Ben Green will take the time to discuss in detail how successful the procedure was and address any questions or concerns you might have. During the surgery, a skilled pathologist will be present to assist in the evaluation of any tissues removed. If Dr. Green identifies an abnormal parathyroid gland during the procedure, he will remove it and ensure it is carefully examined under a microscope to confirm its condition. This process is considered a highly reliable and effective procedure. In the next day or two, the gland will undergo a thorough assessment to ensure accurate results. A few hours post-surgery, a blood test will be conducted to check your parathyroid hormone (PTH) and calcium levels. If the surgery was successful, these vital levels should return to normal values relatively quickly, indicating a positive outcome.
Is surgery always successful?
The success rate for a single parathyroidectomy is remarkably high, exceeding 85-90%. Most patients who are diagnosed with hyperparathyroidism can have the abnormal gland eliminated successfully in just one surgical procedure. However, it is important to note that a small number of patients may encounter challenges in locating the gland during the initial operation, which may lead to the necessity for additional tests and potential follow-up surgeries. If imaging techniques can accurately identify the abnormal gland prior to surgery, approximately 95% of patients will achieve a successful outcome. Conversely, if the gland cannot be located beforehand, there is a slightly elevated chance that it may not be found during the first operation. Nevertheless, even in these situations, there remains a commendable success rate of over 85% for these cases.
What happens if the abnormal parathyroid gland is not found?
In a few patients, the abnormal parathyroid gland may not be found during the first surgery. The parathyroid glands are usually in predictable locations, often symmetrical on both sides of the neck. The upper parathyroid glands are typically found where expected 80% of the time, while the lower glands can vary. Only 50% of the time are they found behind the lower part of the thyroid. The lower gland may also move into the neck or chest or remain near the skull if it hasn’t descended during development. If the first surgery is unsuccessful, previous imaging will be repeated, and additional tests like a 4D CT scan specifically for the parathyroids may be ordered. In rare cases where imaging does not help, an invasive test called ‘selective venous sampling’ may be done. This involves placing a catheter in the neck veins through the arm to take blood samples, identifying which veins have high PTH levels to assist the surgeon in locating the gland.
What are the potential complications of parathyroid surgery?
Parathyroidectomy is a common surgery that Dr. Green is well-trained to perform. Most patients recover as expected and can leave the hospital feeling good the day after surgery. However, some patients may experience significant complications. Below, you will find a list of potential problems related to breast surgery. Some complications are common, while others are rare but serious. This list is just a guide and not complete. If you have questions after your consultation or after reading this, please feel free to talk to Dr. Green.
Common (10-20%)
Temporary swelling in neck, with feeling something is stuck.
Bruising, scaring.
Temporary Stiff neck.
Uncommon. (up to 5% of cases)
Wound infection.
Bleeding requiring a second operation.
Temporary nerve palsy – hoarse voice.
Abnormal gland not able to be found (up to 15% in non-localized glands).
Permanently low calcium (up to 20% if 3 ½ glands are removed).
Rare but important (up to 1% of cases)
Major bleeding.
Recurrent laryngeal nerve injury – Hoarse voice.
Permanent low calcium needing supplements.
Anesthetic complications.